"In new research published by the Mercatus Center, I analyze the causes and impact of the much higher-than-expected enrollment and spending associated with the Affordable Care Act (ACA) Medicaid expansion. Though unpredicted by Washington experts, the results were predictable. The federal government’s 100% financing of state spending on expansion enrollees has led states to boost enrollment and create high payment rates. (See this 2-minute Mercatus video for additional information on this significant development.)
In states that have expanded, enrollment and per enrollee spending are nearly 50% higher than predicted. While interest groups within the states—particularly hospitals and insurers—benefit from the higher spending being charged to federal taxpayers, substantial evidence suggests much of this new spending is wasted or provides little value for its intended recipients.
An important 2015 study showed that Medicaid expansion enrollees obtain low value through the program. Moreover, an increasing amount of spending on the program is lost to waste, fraud, and abuse. The Wall Street Journal highlighted a new government report showing that improper Medicaid spending exploded between 2013 and 2016. Improper payments amounted to about $67 billion in 2016, a $41 billion increase from the estimated $26 billion in 2013. The large increase in improper Medicaid payments has occurred while the ACA Medicaid expansion took effect, suggesting that the expansion is the main cause of the stunning rise. (Interestingly, the Department of Health and Human Services has pulled the report from the Internet.)
Perverse Incentives Produce Lots of Waste
Under the ACA, the federal government reimburses 100% of state spending on expansion enrollees—non-disabled, working-age adults with income between the state’s previous eligibility thresholds and 138% of the federal poverty level ($16,394 in 2016). After this year, the federal share gradually phases down until 2020 when it reaches 90%, where it is scheduled to remain.
Common sense suggests that a jurisdiction is more likely to increase spending on an area when the costs can largely be passed to other jurisdictions. This type of financing structure also lessens a jurisdiction’s incentive to ensure that the spending provides high value with low amounts of waste.
ACA Medicaid Explosion
Medicaid, already on an unsustainable cost-growth trajectory before the ACA, has experienced unprecedented enrollment and spending growth since 2013. Medicaid spending in 2015 was nearly $100 billion above the 2013 amount.
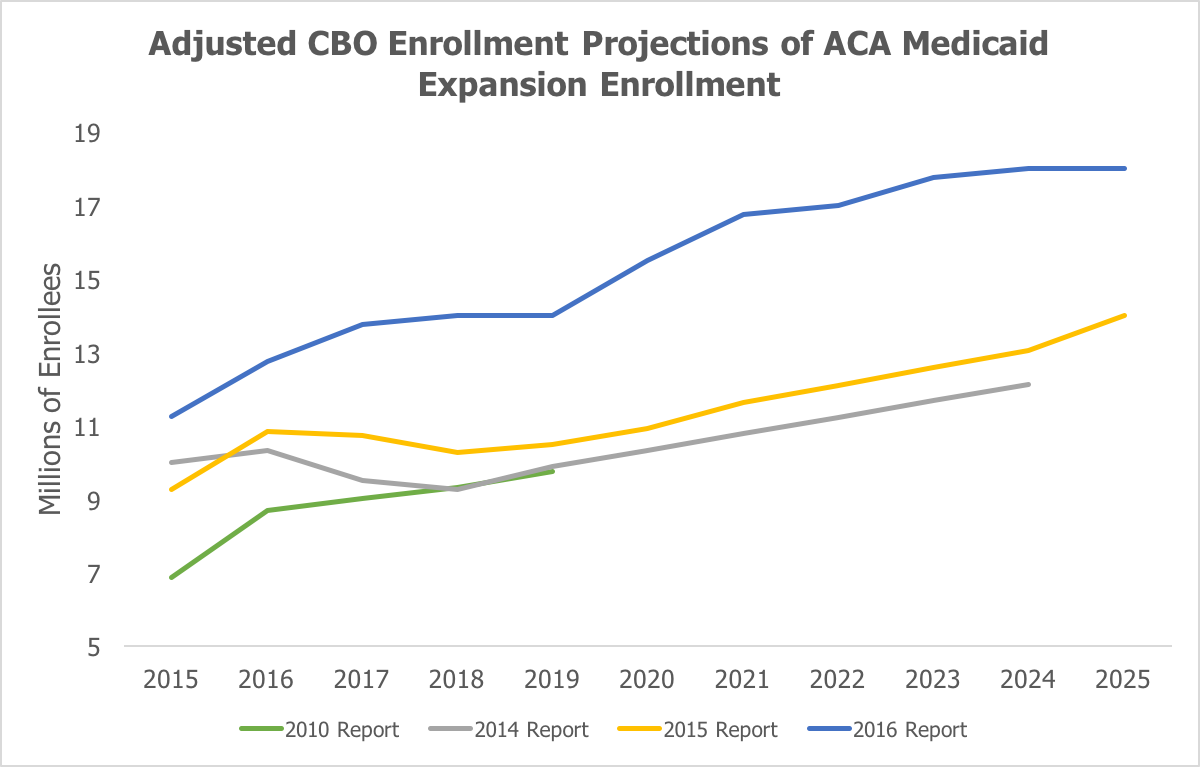
Medicaid expansion enrollment and spending is higher than projected even though not as many states as expected have adopted the expansion. My research shows the difference in the Congressional Budget Office’s (CBO) Medicaid expansion enrollment and spending projections over time. The first figure shows CBO’s most recent estimate of expansion enrollment along with CBO’s estimates from 2010, 2014, and 2015.
Enrollment is much higher than CBO expected when the ACA passed in 2010, and it is also significantly higher, particularly in 2017 and beyond, than estimated in both CBO’s 2014 and 2015 reports. Essentially, this means that far more people—roughly 50% more—have enrolled and are projected to enroll in Medicaid in the states that expanded than was expected by CBO previously. In addition to higher-than-expected enrollment, spending per newly eligible Medicaid enrollee is much greater than expected. As I wrote in July when the Obama administration released the 2015 Medicaid actuarial report, government spending on newly eligible enrollees equaled about $6,366 in 2015—an amount 49% higher than its projection of $4,281 from just one year earlier.
Both higher-than-expected enrollment and spending per enrollee has resulted in the Medicaid expansion being much more costly than projected. For example, in April 2014, CBO projected that the Medicaid expansion would cost $42 billion in 2015. The actual cost was $68 billion, about 62% higher.
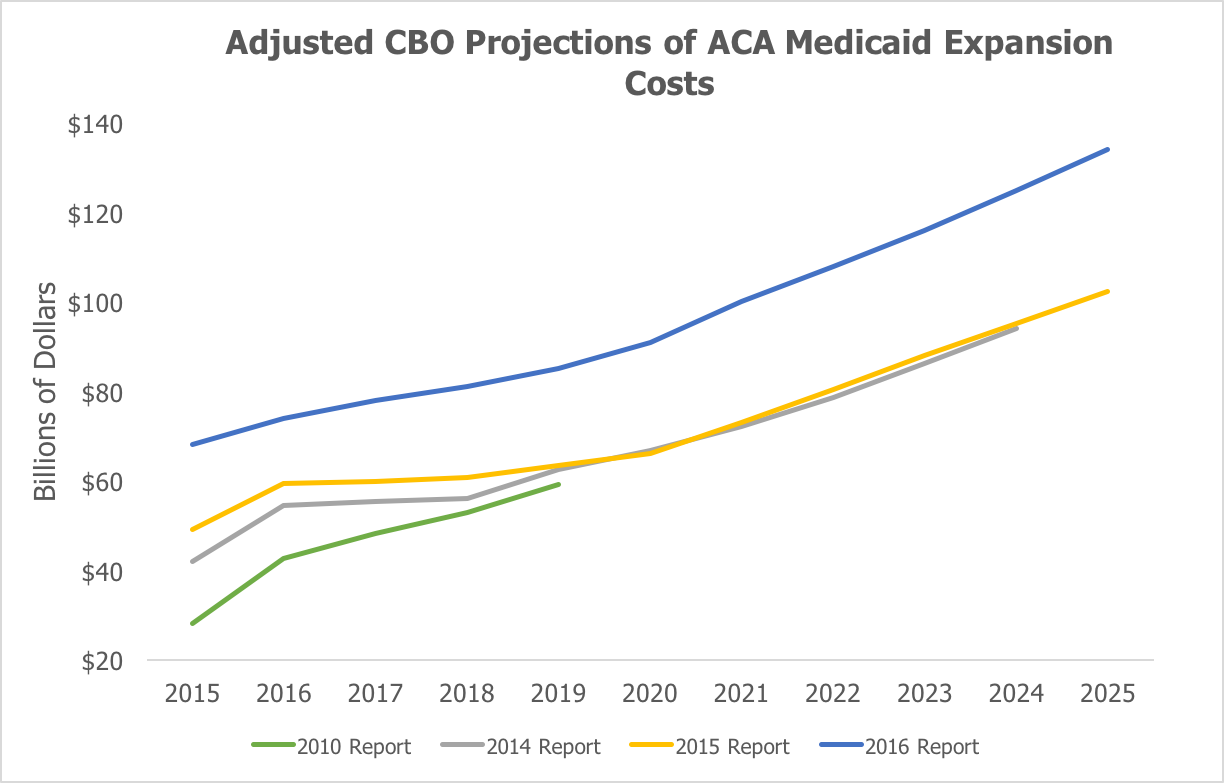
The second figure shows CBO’s projections of federal spending on the Medicaid expansion and how CBO’s most recent projection of the cost are substantially above previous expectations.
Using CBO’s current projections of state adoption of the expansion for its previous estimates shows that federal Medicaid spending between 2016 and 2024 is $232 billion in excess of its April 2014 estimates.
Both figures adjust CBO’s previous year estimates for its current assumptions about state adoption of the expansion. CBO now expects states to adopt the expansion at a slower rate than it has previously projected. In 2010, before the Supreme Court made Medicaid expansion optional for states, CBO expected all states would adopt the expansion. This adjustment allows for a better comparison of enrollment and spending because it holds constant CBO’s assumptions about the percentage of the newly eligible Medicaid population residing in expansionary states.
Too Little Value from Medicaid Expansion
Prior to the ACA, when states shouldered their traditional share of Medicaid spending (an average of 43%), only Vermont and the District of Columbia concluded that the tradeoffs—higher state taxes and reduced spending elsewhere—justified expanding Medicaid to the ACA expansion population. It turns out that states that did not expand Medicaid prior to the ACA almost certainly made a wise cost-benefit calculation.
A 2015 study from economists at Harvard, MIT, and Dartmouth, assessing an earlier Medicaid expansion in Oregon to a similar population to the ACA expansion, found that “[a]cross a variety of alternative specifications … Medicaid’s value to recipients is lower than the government’s costs of the program, and usually substantially below.” They estimated that the “welfare benefit to recipients from Medicaid per dollar of government spending range from about $0.2 to $0.4.” Oregon Medicaid expansion enrollees did not have significant improvements in blood pressure, cholesterol, or blood sugar relative to people who did not enroll in Medicaid.
Reform Medicaid, Stop Viewing Program as Economic Stimulus
In order to increase the value that enrollees receive from Medicaid and lessen the amount lost to waste, fraud, and abuse, it is necessary to change the central incentives underlying the federal-state partnership. In particular, the incentives of the ACA’s elevated reimbursement rate lead policymakers to view Medicaid as an engine for economic stimulus instead of as a welfare program. For example, according to the White House:
“By expanding Medicaid, States can pull billions in additional Federal funding into their economies every year, with no State contribution over the next three years and only a modest one thereafter for coverage of newly eligible people.”
A study by Deloitte Consulting and the University of Louisville projects that the ACA’s Medicaid expansion will add 40,000 jobs and $30 billion to Kentucky’s economy through 2021. The problem with this and similar studies is that they assess the decision of a state in isolation without factoring in other states’ decisions regarding expansion. For example, Kentucky is worse off when other states expand, because her citizens pay federal taxes to finance health benefits that accrue only to individuals in those other states.
Economist Robert Book points out that the American economy is worse from the ACA expansion “because taxation itself has a negative effect on economic activity, over and above the amount of tax collected.” Book estimates a reduction of $174 billion in economic activity over a 10-year period if all states expand Medicaid. He also estimated a total job loss of more than 200,000 positions from 2014 to 2017 if all states expanded Medicaid.
Sensible Medicaid reform has two central goals: reduce the unsustainable trajectory of spending and produce better outcomes for people most in need. The ACA Medicaid expansion significantly adds to the unsustainable spending trajectory of the program, likely fails to produce health outcomes or value to recipients worth the corresponding cost, and creates a large federal government bias toward nondisabled, working-age adults at the expense of traditional Medicaid enrollees. Moving Medicaid back in the right direction requires ending the ACA’s elevated federal reimbursement rate that has given rise to these problems."
Thursday, May 25, 2017
ACA Medicaid Expansion: A Lot of Spending of Little Value
By Brian Blase of Mercatus.
Subscribe to:
Post Comments (Atom)
No comments:
Post a Comment
Note: Only a member of this blog may post a comment.