Evaluating the free market by comparing it to the alternatives (We don't need more regulations, We don't need more price controls, No Socialism in the courtroom, Hey, White House, leave us all alone)
Monday, May 13, 2024
The rise in reported maternal mortality rates in the US is largely due to a change in measurement
Maternal mortality rates appear to have risen in the last 20 years in the US. But this reflects a change in measurement rather than an actual rise in mortality.
But
researchers have shown that this rise does not represent an actual
increase in the number of women dying in childbirth. Rather, it is the
result of a change in measurement that was gradually introduced in the
US between 2003 and 2017.
This
change wasn’t adopted at a national level in a single moment; that
would have led to a single step-wise change in mortality rates. Instead,
the measurement change was adopted state by state, which led to a gradual rise over 14 years.
This
measurement change has helped to identify more deaths that meet the
criteria for maternal deaths, but has also led to some
misclassification.
The process of determining the cause of death
can be complicated, and in many countries, national statistics from
death certificates tend to miss some maternal deaths. To tackle this,
some countries have used additional systems to identify maternal deaths
that would otherwise be unreported.
In this article, I explain how a change in measurement in the United States led to an apparent rising trend in maternal deaths.
The recent rise in reported US maternal mortality looks alarming
Maternal mortality refers to the death of mothers from pregnancy, childbirth, abortion, or related causes.
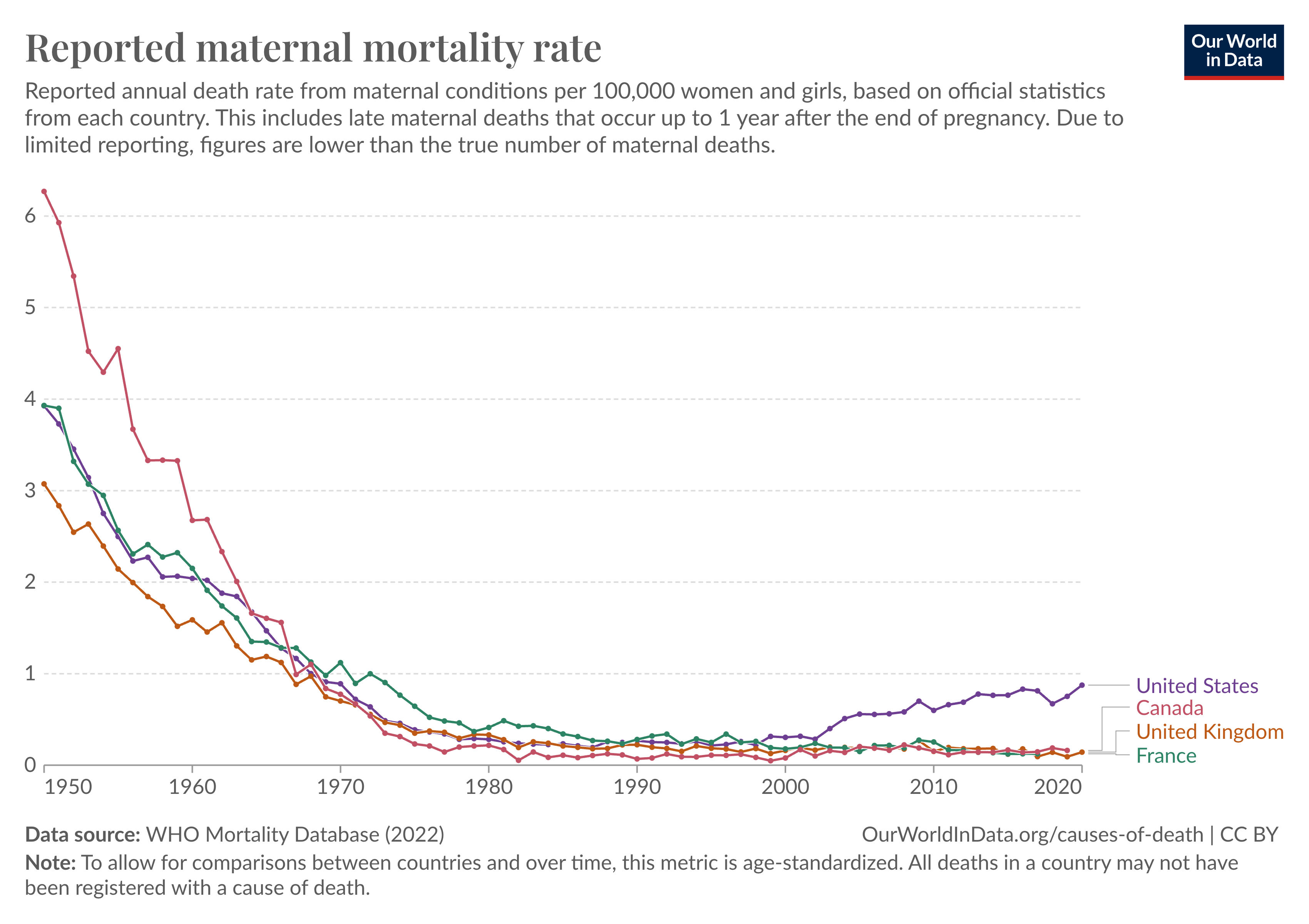
The
chart below shows trends in reported maternal mortality rates between
different countries. Rates are measured as the number of maternal deaths
per 100,000 women in the population. It shows the statistics as
reported to the World Health Organization.1
You can see that the maternal mortality rate has fallen across all of these countries since 1950.
But
in the last two decades, the rate appears to have risen steeply in the
United States. Between 2003 and 2017, it has more than doubled, from 0.4
to 0.8 deaths per 100,000 women.
In other countries such as France, Canada, and the United Kingdom the rates were stable or slightly falling.
Maternal deaths had previously been underestimated
This
cause of death is filled into the field of the death certificate by
doctors and nurses, based on the circumstances of death and medical
records, according to their medical knowledge. The cause of death is
then reported in the country’s vital registry.
You can read more about how causes of death are determined in my article:
But research has found that data from death certificates often underestimates maternal deaths.2
One
reason is that some maternal deaths are missed and attributed to other
causes. This can happen because pregnancy can worsen pre-existing
conditions, such as HIV/AIDS and cardiovascular diseases, and thereby indirectly lead to a woman’s death.3
In these cases, it can be difficult for doctors to make a judgment call
on whether the woman would have died if she had not been pregnant.4
To
complicate the situation further, sometimes medical records are lacking
or inaccessible, and many deceased women don’t have linked hospital
records or undergo an autopsy to confirm whether they were pregnant at
the time of death.5
There can also be social, cultural, or legal issues around reporting whether women were pregnant when they died.
To address these problems, which can lead to the underestimation of maternal deaths, the International Classification of Diseases (ICD)
expanded its definition of maternal deaths and recommended that
countries collect additional data on whether deceased women had been
pregnant before their death.
In
the ninth edition, known as ICD-9 (published in 1979), the definition
of maternal mortality was very narrow: it focused only on deaths during childbirth or the postpartum period, and considered any causes related to, or aggravated by, the pregnancy or its management.
The updated ICD-10 (published in 1994) expanded the definition. It considered all those deaths as maternal which happened during pregnancy, childbirth, or within 42 days of the end of pregnancy, from any cause related to or aggravated by the pregnancy or its management, but not from accidental or incidental causes.6
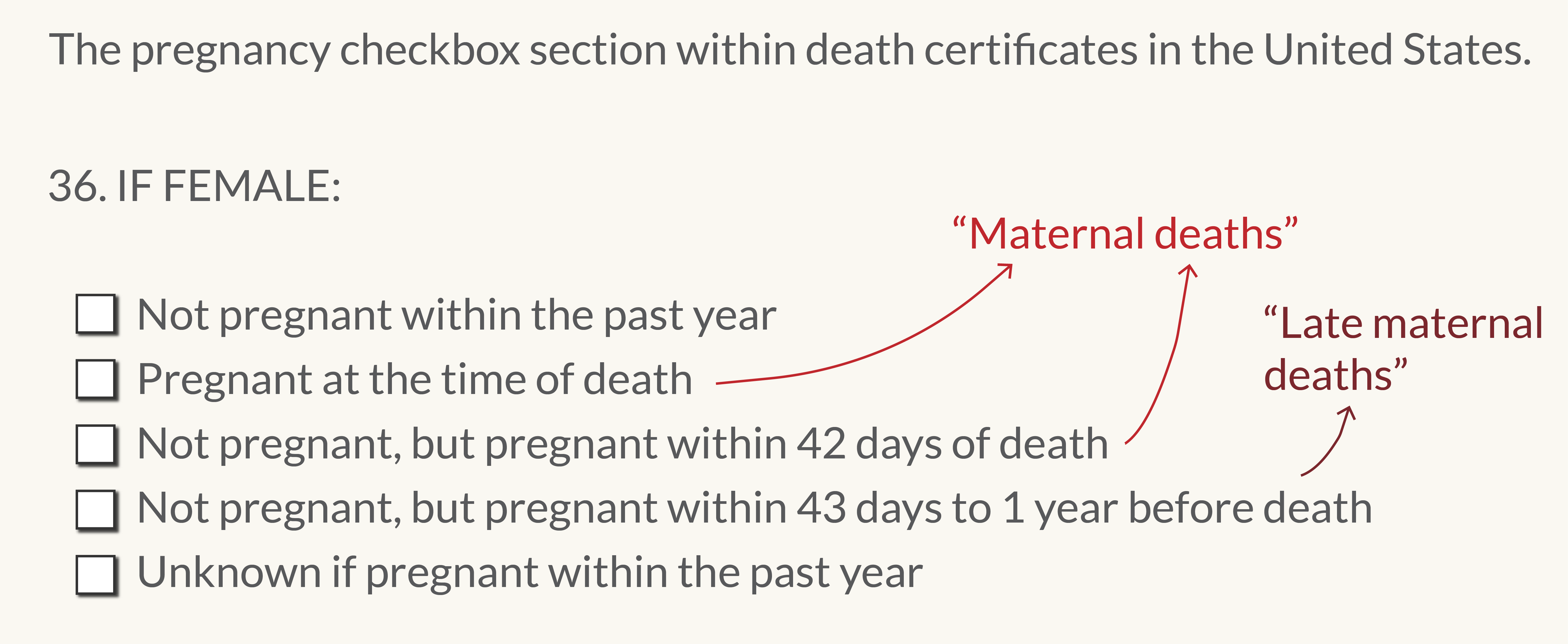
The
ICD-10 also recommended that a “pregnancy checkbox” be included in
national death certificates, which would help flag these deaths for
further investigation to understand if they were caused by pregnancy.
The
checkbox asked if the deceased woman was pregnant or had been recently
pregnant. You can see an example below, which is used in death
certificates in the United States.
This checkbox was introduced to reduce underestimation and to capture maternal mortality more accurately.
The
“pregnancy checkbox” section of death certificates in the United
States. This section was added to death certificates in some states in
2003, and was then gradually adopted across all other US states. The
figure is adapted from Catalano et al. (2020).7
As the checkbox was gradually implemented in the United States, more maternal deaths were reported
To
follow the ICD-10 definition and make sure that maternal deaths weren’t
going uncounted, the United States added the “pregnancy checkbox” to
death certificates, starting in 2003.
The
US used an automated system to code deaths as maternal deaths if the
checkbox was ticked for women between the ages of 10 and 54, regardless
of other information on the death certificate.8
In 2003, four states had implemented the pregnancy checkbox — Idaho, Maryland, Montana, and New York state.9
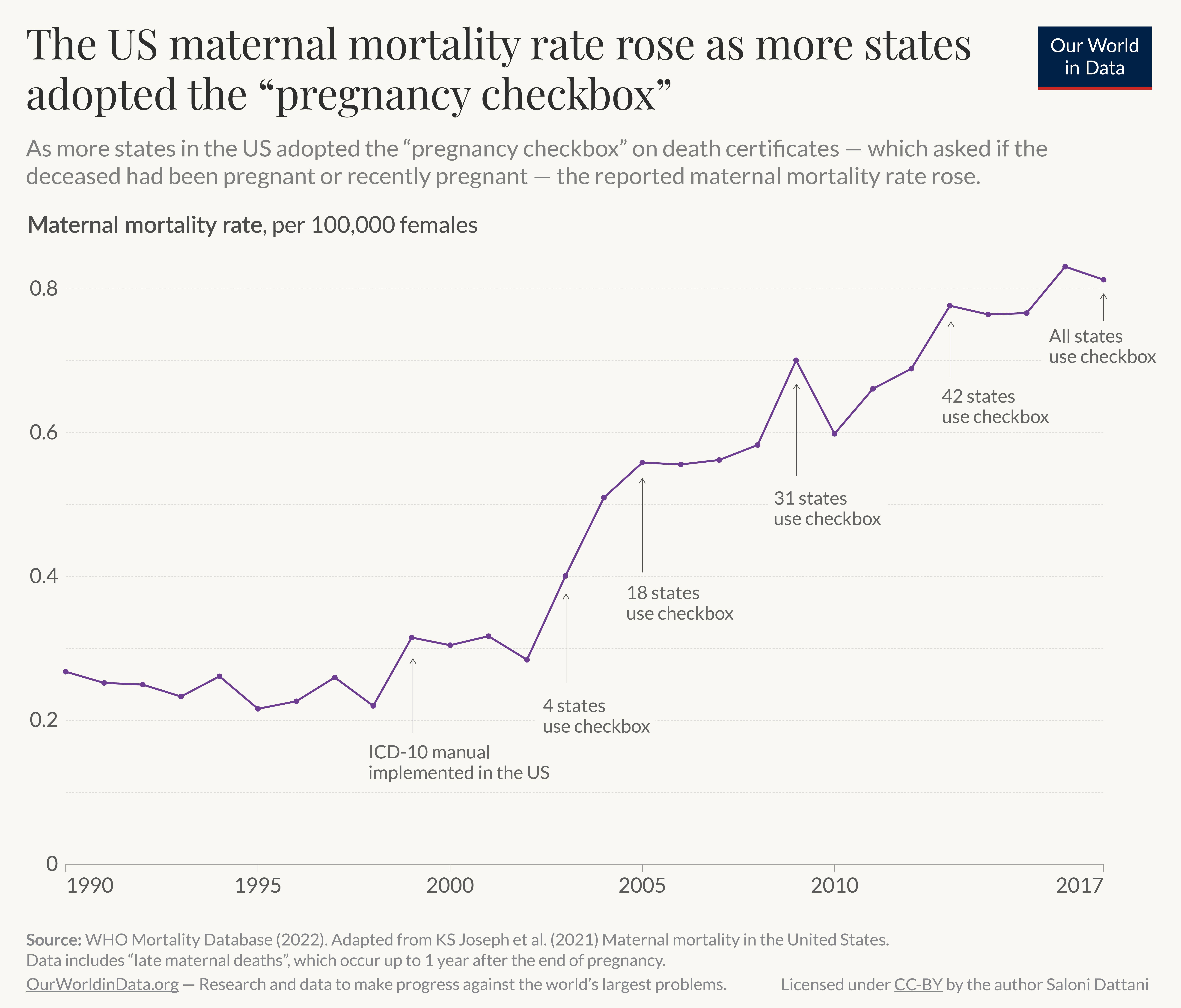
In
the following years, more and more states added the checkbox. It wasn’t
until 2017 that every state included it on death certificates. You can
see this in the chart below.
As
more and more states included the pregnancy checkbox, more deaths were
identified as related to pregnancy, and the reported maternal mortality
rate increased.10
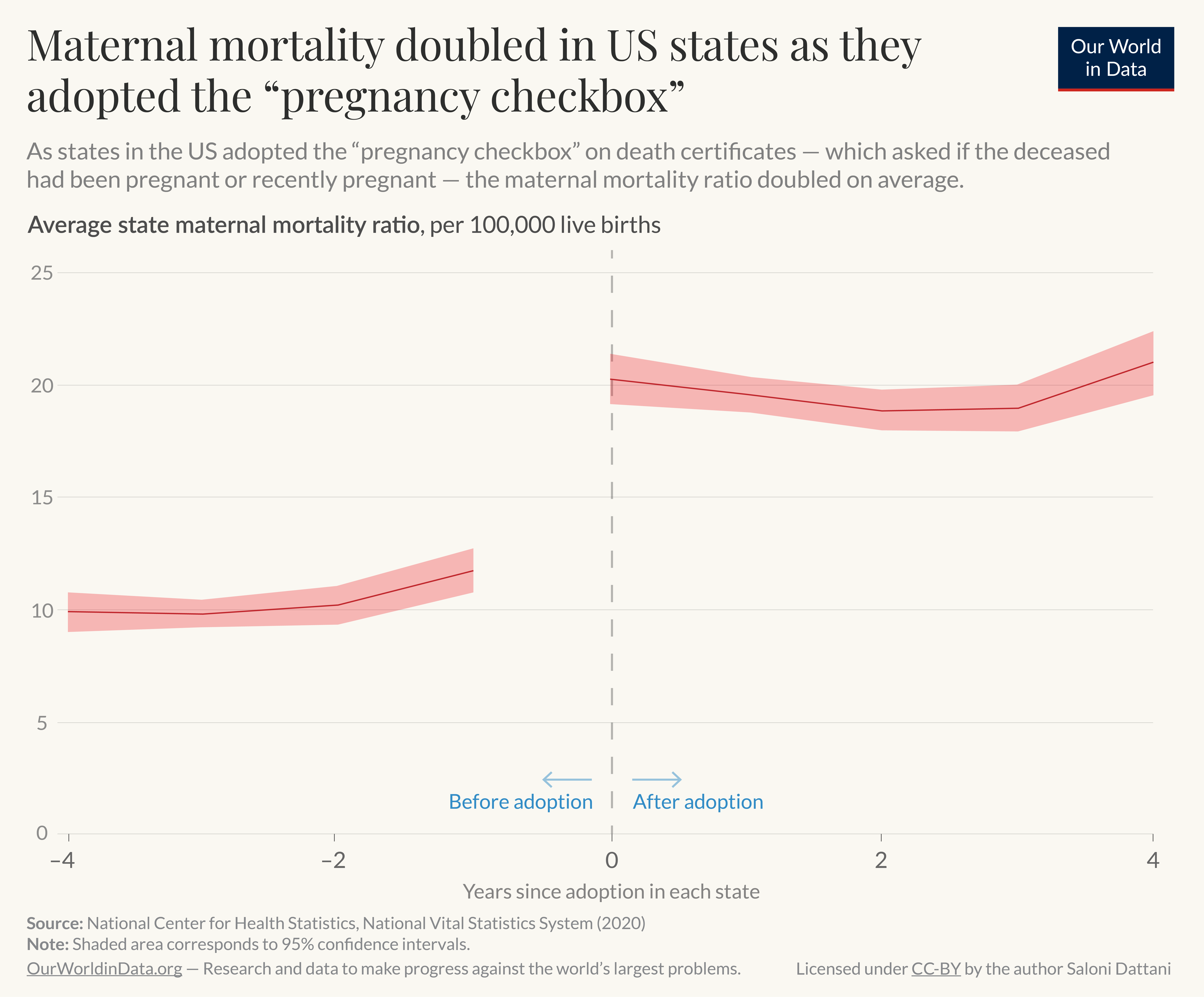
To understand the impact of the measurement change, we can also examine what happened to maternal mortality within states.
This is shown in the chart below, which plots the average maternal mortality ratio before and after the change.
The
chart comes from reports from the National Center for Health Statistics
and the National Vital Statistics System, which is part of the Centers
for Disease Control and Prevention.
You can see that once the checkbox was implemented, the reported maternal mortality ratio suddenly increased — on average, it doubled from 10 to 20 deaths per 100,000 births — and then remained stable.11
The impact of the pregnancy checkbox and misclassification on maternal mortality trends in the United States, 1999–2017.12
The
researchers also estimated what the maternal mortality ratio from 2003
to 2017 would have looked like under two hypothetical scenarios: (a) if
all states adopted the checkbox simultaneously, or (b) if none of them
did.
In both scenarios, they estimate that there would have been no change in maternal mortality ratios between 2003 and 2017.
In other words, the rise in maternal mortality is largely explained by the staggered adoption of the checkbox.13
The researchers also noted that the impact of the change in measurement
was greatest among older women and non-Hispanic black women.
The
checkbox increased the ability to detect pregnancy-related deaths that
would have been missed otherwise, but in some cases, it also resulted in
overcounting deaths from other causes.
In
a quality assurance study of four US states, researchers found that
around 21% of death certificates with the checkbox ticked were confirmed
to be false positives — data from other health systems confirmed they
had not been pregnant, and this was especially the case in girls aged
under 15 and women aged over 45.14 One reason for these false positives is that the box was ticked accidentally in some cases.15
To
reduce these false positives, another change in measurement has been
made in US statistics: from 2018 onwards, the checkbox is disregarded
for women and girls aged under 10 or over 54.16
Researchers
also recommended further quality assurance processes — such as
conducting follow-ups to verify ticked checkboxes and improving training
for death certifiers — to be conducted in other states in the US before sending data to the vital registry, to improve the accuracy of national data on maternal deaths.17
Maternal mortality is underreported in national statistics in many countries
While the United States has used the checkbox to automatically code deaths as maternal if it is ticked18, this practice is not followed in several other countries.19
There is strong evidence that maternal mortality, as defined in the ICD, is underreported in national statistics in many countries.20
One
reason is that some countries do not use data from the checkbox to
identify potential maternal deaths, or do not routinely conduct
additional investigations to identify unreported maternal deaths.19
Some countries have implemented systems separate from their vital registries to investigate potential maternal deaths further.21
These systems include “enhanced surveillance”, which involves an
additional system for more detailed monitoring, and “confidential
inquiries”, which are private investigations into individual cases.
These
investigations have been conducted infrequently, and the maternal
deaths identified through these systems are not necessarily counted in
vital registries for national statistics and given to the WHO.22
Research finds that the number of maternal deaths from vital registries tend to be lower than equivalent definitions from these other surveillance systems.23
In low- and middle-income countries — where death certificates and vital registries are often lacking — other sources of data are used to determine maternal deaths, including hospital records, and verbal autopsies.
Maternal
mortality data from these sources can also include women who have died
from incidental or accidental causes of death that are unrelated to
their pregnancy, because data to identify the specific causes of death
may be lacking.24
International statistics on maternal mortality are adjusted for underreporting, but uncertainties remain
To address this problem — of underreported maternal deaths in vital registries
— the United Nations Maternal Mortality Estimation Inter-agency Group
(MMEIG) uses other data sources and expert knowledge to adjust for
underreporting.
In countries that lack other surveillance systems for maternal deaths, the number of maternal deaths are adjusted upwards.
In
countries that have enhanced surveillance data, different adjustment
factors are used to adjust for incompleteness and misclassification.25
Unfortunately,
this adjustment can be imprecise because many countries lack
comprehensive data on causes of death, or have not conducted national
investigations into unreported maternal deaths, which could be used to
understand the degree of underreporting in each country and improve
adjustment factors.26
Conclusion
To prevent avoidable maternal deaths, it’s crucial to have accurate data on deaths caused by pregnancy and related causes.
Unfortunately,
maternal deaths are often underreported in official statistics due to a
range of reasons, such as missing medical records and poor training of
death certifiers.
To
help identify missed deaths, the United States introduced a “pregnancy
checkbox” on death certificates, and deaths of women with this box
ticked would be coded as maternal deaths in most age groups.
While
this helped identify maternal deaths that would have been missed, it
also led to some misclassification and false positives from women who
had not been pregnant or had died from other incidental causes.
Because
of this, the US changed its coding system in 2018 to disregard the
checkbox for deaths of patients under 10 or over 54 years old.
Researchers
have also recommended that additional quality-assurance measures are
used to verify potential maternal deaths before they are compiled in US
national statistics.
In other high-income countries, there is strong evidence that maternal mortality is underreported in national statistics.
Some
countries rely on additional systems to uncover unreported maternal
deaths, but these tend to be conducted infrequently and are not
necessarily considered in national statistics.
In
contrast, data from low- and middle-income countries — which tend to
lack death certificates, hospital records, and vital registries — are
less precise.
International
organizations try to adjust for these problems of underreporting and
misclassification, but without better surveillance in each country, the
adjustments can be imprecise.
By
improving data collection and surveillance of maternal deaths further,
the world can have a better understanding of where and why mothers are
dying, mobilize resources and policies to save lives, and reduce
maternal mortality further."
No comments:
Post a Comment
Note: Only a member of this blog may post a comment.
No comments:
Post a Comment
Note: Only a member of this blog may post a comment.